Table of Contents
The Mechanics of Emotion Regulation: Dysregulation, Self-Injury, and Clinical Interventions
In clinical psychology, few constructs are as pivotal to mental health as emotion regulation (ER). While the layperson may view emotions as transient feelings, happiness, sadness, or anger, researchers understand them as complex biological and cognitive feedback loops designed to help us navigate our environment. However, when these loops malfunction, we enter the domain of emotion dysregulation, a transdiagnostic risk factor underpinning conditions ranging from Borderline Personality Disorder (BPD) to mood disorders and Non-Suicidal Self-Injury (NSSI).
This article dissects the mechanisms of emotion regulation, the “vicious cycle” of dysregulation, and the specific role of experiential avoidance in self-injury. We will also explore evidence-based strategies for restoring homeostatic balance to the emotional system.
Defining Emotion Dysregulation
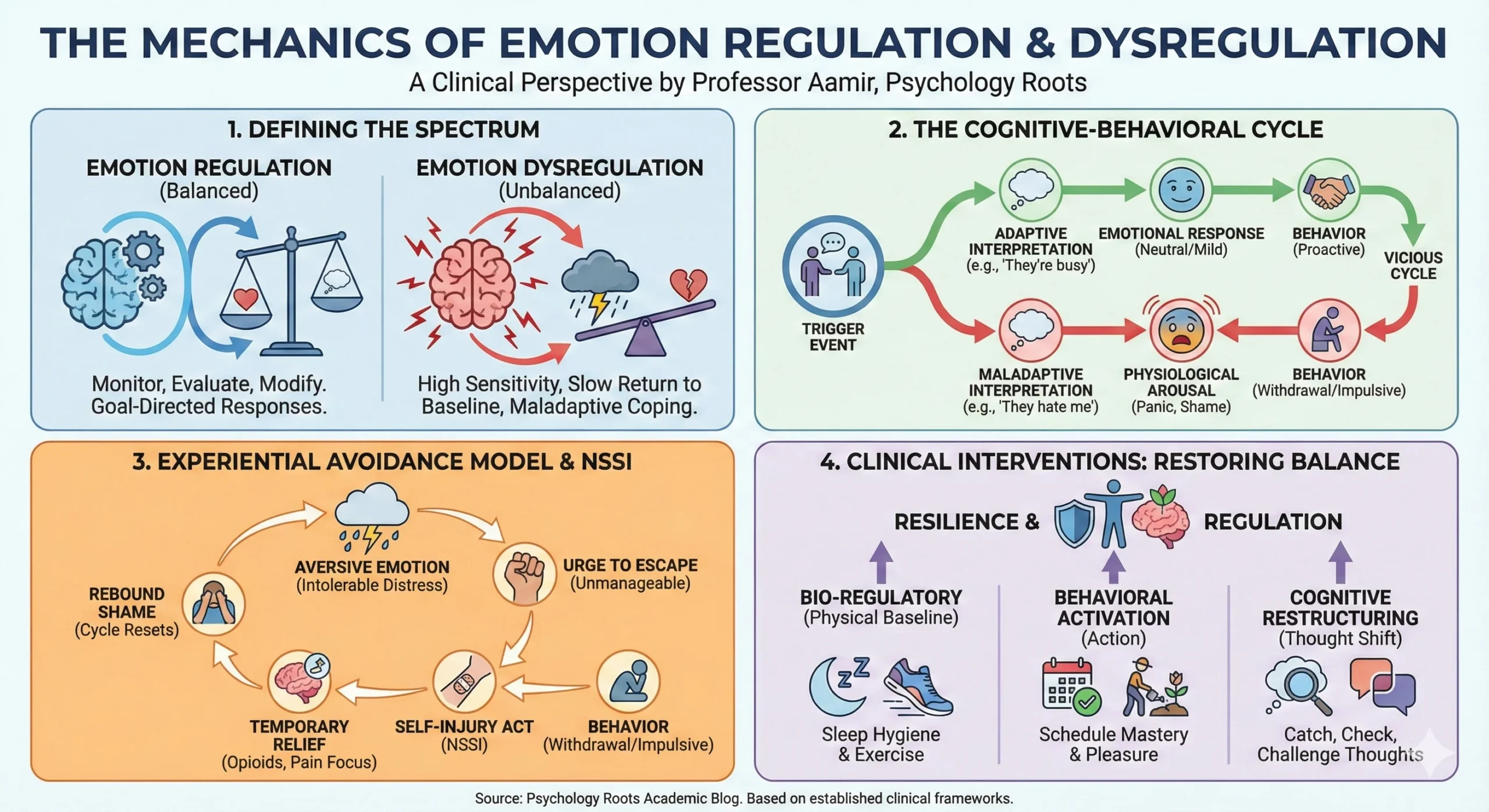
Emotion regulation is not merely the “control” of feelings; it is the ability to monitor, evaluate, and modify emotional reactions to accomplish one’s goals. Conversely, emotion dysregulation is characterized by an inability to manage the intensity and duration of negative affect.
In my clinical experience, patients often describe this state not just as “sadness,” but as an overwhelming physiological storm. Research indicates that dysregulation typically manifests through:
- High Sensitivity: Immediate and intense reactions to stimuli.
- Slow Return to Baseline: An inability to “calm down” once aroused.
- Maladaptive Coping: The use of strategies that reduce immediate distress but cause long-term harm (e.g., substance use, avoidance, or self-injury).
The Cognitive-Behavioral Cycle
The relationship between our internal state and external reality is often mapped using a Cognitive Behavioral Therapy (CBT) framework. A precipitating event (the trigger) does not cause the emotion directly; rather, our interpretation of the event dictates the response.
Example: A friend walks past you without saying hello.
- Adaptive Interpretation: “She must be busy or didn’t see me.” $\rightarrow$ Neutral/Mild Concern.
- Maladaptive Interpretation: “She hates me. I’ve done something wrong.” $\rightarrow$ Panic, Shame, Anger.
This maladaptive interpretation initiates a “vicious cycle” where negative thoughts fuel physiological arousal (racing heart, fatigue), leading to withdrawal or impulsive behavior, which in turn reinforces the original negative thought.
Non-Suicidal Self-Injury (NSSI) and the Experiential Avoidance Model
Why do individuals engage in self-injury? It is a question I am frequently asked by students and parents. The answer lies in the Experiential Avoidance Model (EAM) proposed by Chapman, Gratz, and Brown (2006).
The EAM posits that self-injury is rarely an attempt to die; rather, it is a desperate attempt to regulate intense, unwanted emotional arousal.
The Cycle of Distress
- Stimulus: An interpersonal conflict or triggering event occurs (e.g., rejection).
- Aversive Emotion: The individual experiences intolerable shame, guilt, or anxiety.
- Urge to Escape: The intensity of the emotion feels life-threatening or unmanageable.
- Self-Injury Act: The physical act provides a rapid, sharp physiological jolt.
- Temporary Relief: The body releases endogenous opioids (natural painkillers) and shifts focus from emotional to physical pain, causing a drop in arousal.
- Rebound Shame: The relief is short-lived. The individual then feels shame about the behavior itself, resetting the cycle.
This creates a paradox where the behavior (self-injury) works effectively in the short term (negative reinforcement) but exacerbates the pathology in the long term.
Gender Differences in Emotion Regulation
Research into gender differences suggests that while men and women experience similar emotional frequencies, their regulatory strategies often differ due to socialization and neurodevelopmental factors.
- Internalizing vs. Externalizing: Females often report higher rates of internalizing symptoms (depression, anxiety) and rumination—repetitively focusing on distress. Males are often socialized to suppress vulnerability, leading to externalizing behaviors (aggression, substance use).
- Rumination vs. Reflection: It is critical to distinguish between rumination (passive, repetitive dwelling on negative feelings) and reflection (active processing to gain insight). While women are statistically more prone to rumination, they are also more likely to engage in adaptive reflection, which can be a protective factor.
- Adolescent Vulnerability: Adolescence is a critical window. Females tend to report higher interpersonal stress (friendships), whereas males often report performance-based stress (school/athletics).
Clinical Interventions: Restoring Regulation
Restoring emotion regulation capacity requires a multimodal approach, targeting the body, behavior, and cognition.
1. Bio-Regulatory Strategies (The Physical Baseline)
One cannot regulate emotions with an exhausted nervous system. Basic physiological needs—often ignored in crisis—are foundational.
- Sleep Hygiene: Sleep deprivation significantly lowers the threshold for emotional reactivity.
- Physical Activity: Exercise metabolizes stress hormones (cortisol) and increases endorphins, providing a “buffer” against dysregulation.
2. Behavioral Activation
Depression and dysregulation feed on withdrawal. Behavioral Activation involves scheduling activities that provide a sense of Mastery (achievement) or Pleasure. Even small acts, like cleaning a room or finishing a minor task, can disrupt the loop of helplessness.
3. Cognitive Restructuring
Changing how we feel is difficult; changing how we think is more accessible. This involves “catching” automatic negative thoughts and subjecting them to scrutiny.
- The Check: “Is this thought a fact, or an interpretation?”
- The Challenge: “What evidence do I have for and against this thought?”
- The Shift: “How important will this be in one week, one month, or one year?”.
Conclusion
Emotion dysregulation is not a character flaw; it is a skills deficit. Whether through therapy, mindfulness, or lifestyle changes, the goal is to widen the gap between the trigger and the response, allowing for a choice rather than a reflex. By understanding the mechanics of the “vicious cycle” and the function of behaviors like self-injury, clinicians and individuals can move from reactive suffering to proactive resilience.
Would you like me to develop a specific worksheet on “Cognitive Restructuring” for your students or clients?
References
- Chapman, A. L., Gratz, K. L., & Brown, M. Z. (2006). Solving the puzzle of deliberate self-harm: The experiential avoidance model. Behaviour Research and Therapy, 44(3), 371-394.
- Duggan, J. M., Toste, J. R., & Heath, N. L. (2013). An examination of the relationship between body image factors and non-suicidal self-injury in young adults: The mediating influence of emotion dysregulation. Psychiatry Research, 206(2-3), 256-264.
- Hilt, L. M., Hanson, J. l., & Pollak, S. D. (2011). Emotion Dysregulation. Encyclopedia of Adolescence, 3, 160-169.
- Macklem, G. L. (2008). Practitioner’s Guide to Emotion Regulation in School-Aged Children. Springer.
- Robinson, A. L., Mansfield-Green, S., & Lafrance, G. (2014). Disordered eating behaviours in an undergraduate sample: Associations among gender, body mass index, and difficulties in emotion regulation. Canadian Journal of Behavioural Science, 46(3), 320-326.
- Rolston, A., & Lloyd-Richardson, E. (n.d.). What is emotion regulation and how do we do it? Cornell Research Program on Self-Injury and Recovery.