Table of Contents
History of Couple Therapy: A Millennial Review of Theory & Practice
The practice of couple therapy, while often perceived as a modern development, possesses a history characterized by fragmentation, theoretical shifts, and a struggle for professional identity. Historically, the field has been viewed through a “developmental” metaphor – initially seen as an infant discipline, then an adolescent full of undirected energy, and finally reaching young adulthood. However, such metaphors often obscure the complex reality of the field’s evolution.
A rigorous historical analysis reveals that couple therapy has progressed through four distinct conceptual phases, moving from atheoretical counseling to a sophisticated, integrated discipline that plays a crucial role in public health. This article provides a critical review of these phases, analyzing the theoretical refinements and the ironic “return of the self” that characterizes contemporary practice.
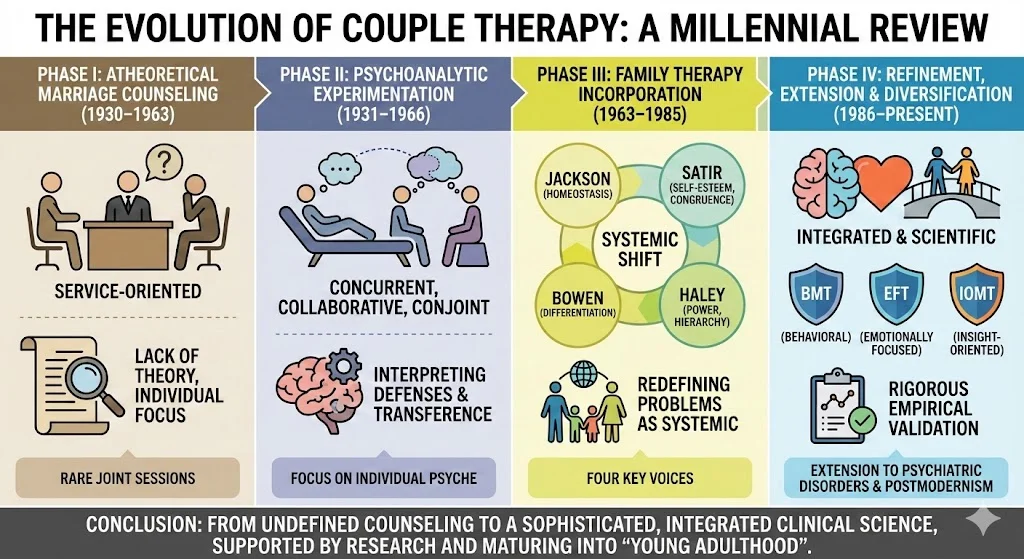
Phase I: Atheoretical Marriage Counseling Formation (1930–1963)
The genesis of couple therapy lies in the “marriage counseling” movement, which began organizationally around 1930. During this “Pioneer” and subsequent “Establishment” stage, practitioners were largely service-oriented, often clergy or gynecologists, rather than mental health professionals.
The defining characteristic of this phase was its lack of theoretical foundation. It was described as a “technique in search of a theory”. Counseling was didactic, short-term, and focused on providing information rather than psychotherapeutic intervention. Paradoxically, despite the focus on the dyad, early marriage counselors rarely employed conjoint sessions. In the 1940s, only 5% of cases involved joint interviews; this number rose slowly to 15% by 1960. The transition to conjoint therapy was sluggish, and when counselors eventually sought a theoretical anchor, they turned to psychoanalysis, a move that fundamentally altered the trajectory of the field.
Phase II: Psychoanalytic Experimentation (1931–1966)
While marriage counseling struggled for identity, a parallel movement occurred within psychiatry. Psychoanalytic clinicians, frustrated by the limitations of individual analysis for marital problems, began experimenting with concurrent and conjoint formats.
Key developments in this phase included:
- Concurrent Therapy: Treating spouses individually but synchronously. Bela Mittelman was a pioneer here, eventually introducing joint sessions when spouses’ stories conflicted, inadvertently moving toward a systemic perspective.
- Collaborative Therapy: Partners treated by different therapists who communicated to maintain the marriage.
- Conjoint Therapy: The treatment of the couple together. By the 1960s, this became the preferred format, emphasizing the interpretation of defenses and the “working through” of transference within the dyadic relationship.
Despite these advances, this phase was marked by ambivalence. Therapists struggled to reconcile the “real” relationship with the “transferential” relationship, often maintaining a focus on the individual psyche rather than the interactional system.
Phase III: Family Therapy Incorporation (1963–1985)
The third phase represents a radical shift where the emerging field of family therapy effectively “engulfed” marriage counseling. Family therapy pioneers, reacting against individual-oriented psychiatry, redefined marital problems as systemic issues. During this “Golden Age,” four distinct voices shaped the conceptual landscape:
1. Don D. Jackson: The Marital Quid Pro Quo
Jackson, a founder of the Mental Research Institute (MRI), introduced the concept of family homeostasis and the marital quid pro quo. Often misunderstood as a literal “this for that” behavioral exchange, Jackson originally conceptualized the quid pro quo as a metaphorical, often unconscious agreement regarding how partners define themselves in the relationship. His focus was on the “command” aspect of communication and the rules governing interaction.
2. Virginia Satir: Self-Esteem and Congruence
Satir was the leading humanistic figure of the era. Unlike the “systems engineers” of her time, she emphasized self-esteem, congruent communication, and the “self in the system”. She viewed symptoms as defenses against low self-worth and advocated for the therapist as a nurturing resource who modeled clear communication. Her work foreshadowed modern attachment-based approaches.
3. Murray Bowen: Differentiation of Self
Bowen’s theory prioritized differentiation of self—the ability to distinguish between thoughts and feelings and to remain autonomous while intimate. He viewed marital conflict as a symptom of emotional fusion and anxiety, often involving “triangulation” (recruiting a third party to stabilize the dyad). Therapy focused on the individual’s ability to “detriangulate” and manage anxiety, rather than teaching interactional skills.
4. Jay Haley: Power and Hierarchy
Haley introduced a strategic perspective, viewing marriage as a struggle for power and control. He rejected the value of insight and the expression of feelings, arguing instead for direct intervention to alter dysfunctional hierarchies. His approach was pragmatic and directive, using paradox and reframing to disrupt maladaptive patterns.
Phase IV: Refinement, Extension, Diversification, and Integration (1986–Present)
The current phase is characterized by a resurgence of couple therapy as a distinct and scientifically rigorous discipline. It involves the refinement of clinical models, the extension of therapy to psychiatric disorders, and a diversification of perspectives.
Refinement of Clinical Models
Three major traditions have solidified their empirical bases during this period:
- Behavioral Marital Therapy (BMT): Evolving from simple “behavior exchange” models, BMT now incorporates cognitive factors and “acceptance” strategies (Integrative Behavioral Couple Therapy), addressing the limitations of skills-based training.
- Emotionally Focused Therapy (EFT): Grounded in attachment theory, EFT focuses on restructuring the emotional bond between partners. It emphasizes the accessing of unacknowledged feelings and the creation of a secure base.
- Insight-Oriented Marital Therapy (IOMT): This approach revitalized psychodynamic thinking, focusing on “affective reconstruction” and the interpretation of unconscious relational themes derived from developmental history.
Extension to Psychiatric Disorders
Couple therapy has extended beyond relationship conflict to treat individual psychopathologies. Research supports its efficacy in treating depression (particularly in women), anxiety disorders (agoraphobia), and alcoholism. The systemic perspective posits that marital distress often maintains or exacerbates these conditions, making conjoint treatment a vital component of comprehensive care.+2
Diversification and Postmodernism
The field has also been reshaped by feminism, multiculturalism, and postmodernism. Feminist critics like Goldner and Hare-Mustin challenged the systemic notion of “circularity” in cases of violence and highlighted the impact of gendered power dynamics. Similarly, multicultural perspectives necessitate an ethnographic approach, respecting the unique cultural matrix of each couple.+3
Critical Analysis: The Great Historical Ironies
A review of this history reveals significant ironies that define the current state of the field.
- The Return of the Individual: During the “systems purist” era (Phase III), the individual psyche was largely ignored in favor of interactional mechanics. Contemporary couple therapy has ironically become more systemic by re-including the individual—acknowledging intrapsychic factors, biological dispositions, and individual psychopathology.
- The Origins of Innovation: Despite the dominance of family systems theory, the most effective modern couple therapies (EFT, BMT) originated not from “pure” family therapy schools but from traditional psychological theories—social learning, attachment theory, and psychodynamics.
- Scientific Rigor: Once a field with “no data”, couple therapy has developed a robust research base. Efficacy studies consistently demonstrate that couple therapy produces large effect sizes, comparable to or exceeding those of individual psychotherapy.
Conclusion
Couple therapy has matured from an undefined counseling activity into a sophisticated clinical science. The integration of individual and systemic perspectives, supported by rigorous empirical validation, marks its current “young adulthood.” For the clinician, understanding this history is not merely an academic exercise; it is essential for navigating the complex interplay of behavior, emotion, and history that defines the couple relationship.
References
- Alexander, J.F., Holtzworth-Munroe, A., & Jameson, P. (1994). The process and outcome of marital and family therapy: Research review and evaluation. In A.E. Bergin & S.L. Garfield (Eds.), Handbook of psychotherapy and behavior change (4th ed., pp. 595-630). John Wiley & Sons.
- Bowen, M. (1978). Family therapy in clinical practice. Jason Aronson.
- Broderick, C.B., & Schrader, S.S. (1991). The history of professional marriage and family therapy. In A.S. Gurman & D.P. Kniskern (Eds.), Handbook of family therapy (Vol. 2, pp. 3-40). Brunner/Mazel.
- Fraenkel, P. (1997). Systems approaches to couple therapy. In W.K. Halford & H.J. Markman (Eds.), Clinical handbook of marriage and couples interventions (pp. 379-414). John Wiley & Sons.
- Gottman, J.M. (1999). The marriage clinic: A scientifically based marital therapy. W.W. Norton.
- Gurman, A.S. (2002). The history of couple therapy: a millennial review. Family Process.
- Gurman, A.S., & Jacobson, N.S. (Eds.). (2002). Clinical handbook of couple therapy (3rd ed.). Guilford Press.
- Haley, J. (1963). Marriage therapy. Archives of General Psychiatry, 8, 213-234.
- Jackson, D.D. (1965). Family rules: The marital quid pro quo. Archives of General Psychiatry, 12, 589-594.
- Johnson, S.M. (1996). The practice of emotionally focused marital therapy. Brunner/Mazel.
- Satir, V. (1964). Conjoint family therapy. Science and Behavior Books.