Table of Contents
Obsessive-Compulsive Disorder (OCD): Etiology, Symptoms, and Evidence-Based Treatment
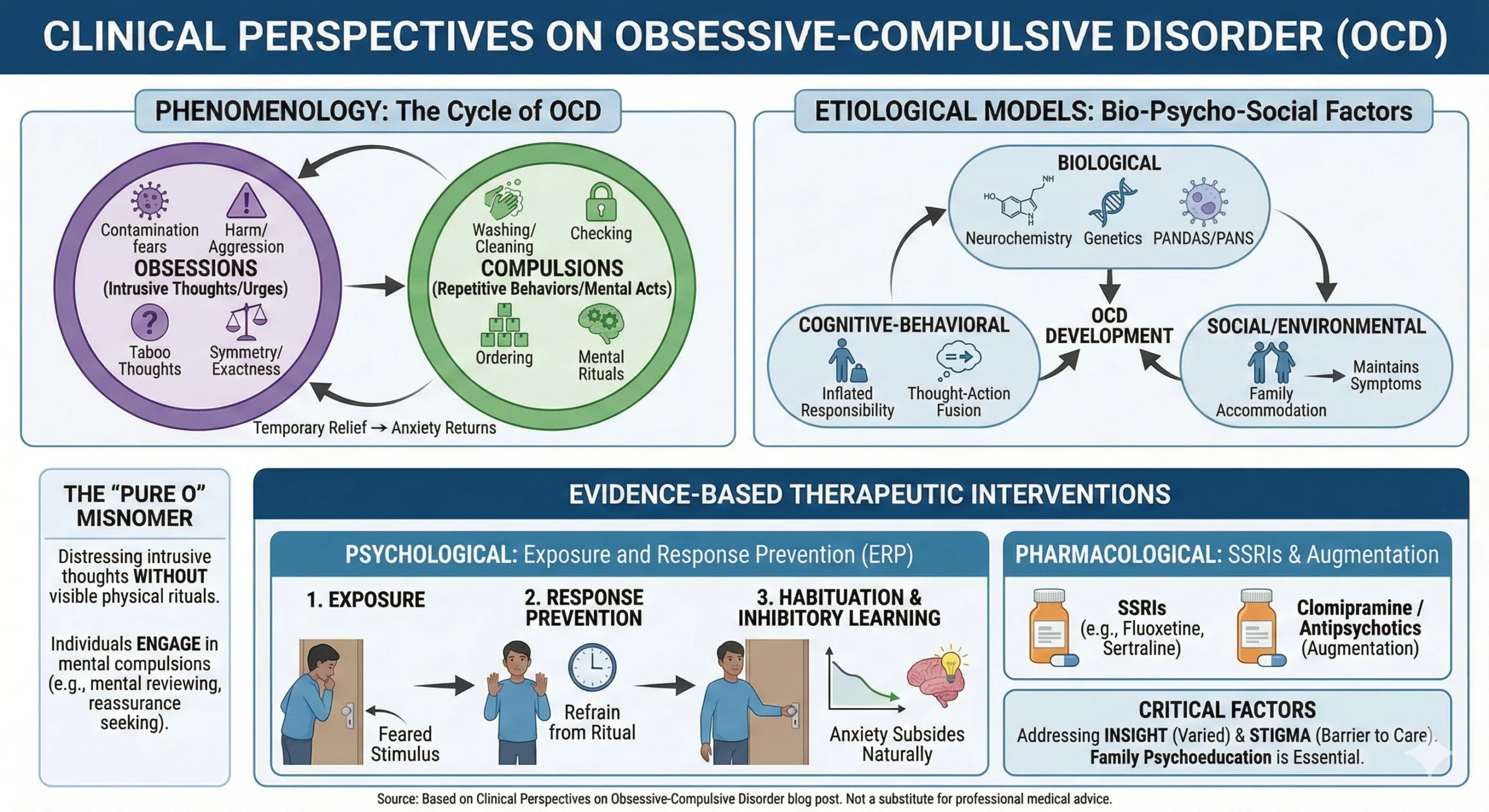
Obsessive-Compulsive Disorder (OCD) is a chronic and debilitating neuropsychiatric condition characterized by the cyclical interaction of intrusive, distressing thoughts (obsessions) and repetitive behaviors or mental acts (compulsions) aimed at reducing the associated anxiety. While historical conceptualizations often trivialized the disorder as a mere “neurosis” or “preference for order,” contemporary clinical psychology recognizes OCD as a severe anxiety disorder that significantly impairs psychosocial functioning and quality of life.
Epidemiological data suggests that OCD affects a significant portion of the population, often manifesting with a bimodal onset in late childhood or early adulthood. The disorder is distinct from Obsessive-Compulsive Personality Disorder (OCPD), a differentiation that is clinically crucial yet frequently misunderstood by lay populations. This article provides a comprehensive overview of the phenomenology, biological underpinnings, and evidence-based management of OCD, serving as a resource for students, clinicians, and researchers.
Phenomenology of the Disorder
The diagnostic criteria for OCD hinge on the presence of obsessions, compulsions, or both, which consume more than one hour per day or cause clinically significant distress.
1. Obsessions
Obsessions are defined as recurrent, persistent thoughts, urges, or images that are experienced as intrusive and unwanted (ego-dystonic). Unlike the worries associated with Generalized Anxiety Disorder (GAD), which typically focus on real-life problems, OCD obsessions are often bizarre or irrational in content. Common themes include:
- Contamination: Fears of germs, dirt, or environmental toxins.
- Harm/Aggression: Fear of acting on an impulse to harm oneself or others (e.g., pushing someone onto train tracks).
- Taboo Thoughts: Intrusive sexual or blasphemous images (e.g., pedophilic fears in non-pedophilic individuals).
- Symmetry/Exactness: A need for objects to be aligned or actions to be performed “just right”.
2. Compulsions
Compulsions are repetitive behaviors or mental acts that the individual feels driven to perform in response to an obsession or according to rigid rules. The function of the compulsion is to reduce distress or prevent a dreaded event, despite the lack of a realistic connection between the action and the outcome.
- Overt Compulsions: Washing, checking (locks, appliances), ordering, and repeating actions.
- Covert (Mental) Compulsions: Silent counting, praying, or mentally reviewing conversations to ensure no harm was caused.
3. The “Pure O” Misnomer
A significant clinical nuance is the concept of “Pure O” (Purely Obsessional). This term is often used to describe patients who report distressing intrusive thoughts without visible physical rituals. However, this is largely a misnomer; research indicates that these individuals almost always engage in mental compulsions or reassurance-seeking behaviors. For example, a patient with intrusive thoughts about infidelity may mentally check their feelings toward their partner repeatedly to “prove” they are still in love.
Etiological Models: Bio-Psycho-Social Perspectives
The etiology of OCD is multifactorial, involving a complex interplay of genetic, neurobiological, and environmental factors.
Biological Factors
- Neurochemistry: The Serotonin Hypothesis posits that dysregulation in serotonergic pathways contributes to symptom severity, supported by the efficacy of Serotonin Reuptake Inhibitors (SRIs). More recent literature also implicates the glutamatergic and dopaminergic systems in the pathophysiology of the disorder.
- Genetics: Twin studies indicate a substantial heritable component, with heritability estimates ranging from 45-65% in pediatric onset and 27-47% in adult-onset cases.
- PANDAS/PANS: In a subset of pediatric cases, sudden-onset OCD symptoms may follow a streptococcal infection (PANDAS) or other immune triggers (PANS), suggesting an autoimmune mechanism affecting the basal ganglia.
Cognitive-Behavioral Factors
Cognitive models suggest that OCD arises not from the intrusive thoughts themselves—which are near-universal in the general population—but from the misinterpretation of these thoughts.
- Inflated Responsibility: The belief that one has the power to prevent or cause negative outcomes and is morally culpable if they fail to intervene.
- Thought-Action Fusion: The belief that thinking about an event increases the likelihood of it happening, or that having a “bad” thought is morally equivalent to doing a “bad” action.
Evidence-Based Therapeutic Interventions
Effective management of OCD requires a structured, multi-modal approach. The “gold standard” interventions are Cognitive Behavioral Therapy (CBT) with Exposure and Response Prevention (ERP) and pharmacotherapy.
1. Exposure and Response Prevention (ERP)
ERP is the most empirically supported psychological treatment for OCD. It operates on the principles of habituation and inhibitory learning.
- Exposure: The patient is systematically exposed to feared stimuli (e.g., touching a doorknob without washing).
- Response Prevention: The patient is guided to refrain from performing the associated ritual (e.g., waiting 30 minutes before washing hands, or not washing at all).
- Mechanism: Over time, the patient learns that the anxiety naturally subsides without the ritual (habituation) and that the feared consequence does not occur (expectancy violation).
2. Pharmacotherapy
First-line pharmacological treatment involves High-Dose Selective Serotonin Reuptake Inhibitors (SSRIs) such as fluoxetine, sertraline, or fluvoxamine. In resistant cases, augmentation with low-dose antipsychotics or switching to clomipramine (a tricyclic antidepressant) may be considered.
3. Family Systems and Accommodation
Family members often inadvertently maintain OCD symptoms through “accommodation”—participating in rituals or providing reassurance to reduce the patient’s distress. Clinical research demonstrates that higher levels of family accommodation correlate with poorer treatment outcomes. Interventions must therefore include family education to gradually withdraw this support in a compassionate manner.
Critical Analysis: The Challenge of Insight and Stigma
A unique challenge in treating OCD is the variance in “insight.” While many patients recognize their fears are irrational (good insight), others may hold their beliefs with delusional intensity (poor/absent insight). This impacts treatment adherence, as patients with poor insight are less likely to engage in the rigors of ERP.
Furthermore, the stigma surrounding intrusive thoughts—particularly those of a sexual or violent nature—creates a significant barrier to care. Patients often endure symptoms for years due to the shame of being labeled “dangerous” or “perverted,” despite the fact that individuals with OCD are no more likely to act on these thoughts than the general population. It is incumbent upon clinicians to normalize the nature of intrusive thoughts to facilitate open disclosure and effective treatment.
Conclusion
Obsessive-Compulsive Disorder is a complex condition that transcends the stereotype of “cleanliness.” It is a disorder of doubt, anxiety, and the desperate need for certainty. However, with the application of rigorous Exposure and Response Prevention (ERP) and appropriate pharmacotherapy, the prognosis for OCD is positive. Early intervention, family psychoeducation, and a reduction in societal stigma are essential components in the pathway to recovery.
References
- Mind. (2016). Understanding obsessive compulsive disorder (OCD). Mind.
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.).
- International OCD Foundation. (n.d.). What Causes OCD?
- Hirschtritt, M. E., Bloch, M. H., & Mathews, C. A. (2017). Obsessive-compulsive disorder: Advances in diagnosis and treatment. JAMA, 317(13), 1358-1367.
- Krebs, G., & Heyman, I. (2015). Obsessive-compulsive disorder in children and adolescents. Archives of Disease in Childhood, 100(5), 495-499.
- Mataix-Cols, D., et al. (2016). A population-based study of the long-term risk of suicide attempts and suicide in obsessive-compulsive disorder. Molecular Psychiatry.