Table of Contents
A Critical Analysis of Pharmacotherapy Versus Psychotherapy in Clinical Practice
The dialectic between pharmacotherapy and psychotherapy remains one of the most persistent debates in clinical psychology. A recent discourse within the professional community highlights a pervasive dichotomy: is medication a necessary stabilizer or a mere “band-aid”? Are psychotherapeutic interventions the only path to genuine “cure,” or do they falter without biological support?. These questions, while seemingly philosophical, have profound implications for treatment outcomes and patient care.
In my tenure supervising clinical trainees, I often observe a tendency to retreat into camps: the “biological determinists” who view mental illness strictly as neurochemical deficits, and the “psychological purists” who view medication as an impediment to emotional processing. However, empirical evidence suggests that adhering to a rigid “versus” framework is not only scientifically outdated but clinically negligent. This article synthesizes qualitative professional insights with rigorous peer-reviewed evidence to establish a comprehensive framework for integrating these modalities.
The Efficacy of Combination Treatment
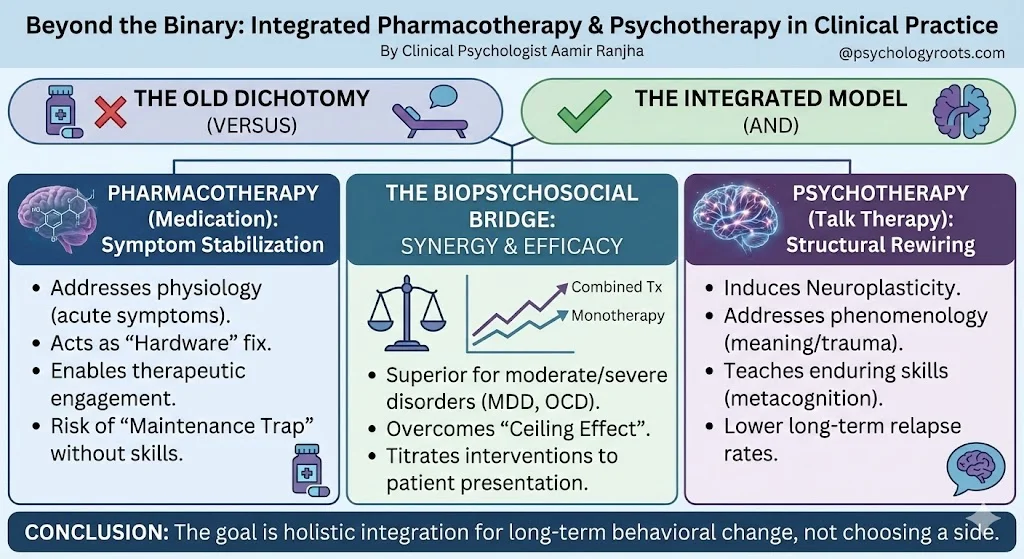
While anecdotal evidence often sways toward individual preference, the data regarding treatment efficacy is robust. The prevailing consensus in high-impact literature aligns with the “additive model,” which suggests that for moderate to severe disorders, the whole is greater than the sum of its parts.
- Superiority in Severity: Meta-analytic reviews consistently demonstrate that combined treatment (pharmacotherapy plus psychotherapy) is statistically superior to monotherapy for Major Depressive Disorder (MDD), Panic Disorder, and Obsessive-Compulsive Disorder (OCD). The standardized mean difference (SMD) often favors combination therapy, particularly in acute phases where symptom severity creates a barrier to cognitive engagement.
- The Ceiling Effect: Interestingly, research indicates a “ceiling effect” for both modalities when used in isolation; neither medication nor therapy alone typically exceeds a 50-60% response rate in intent-to-treat analyses for severe depression. This underscores the necessity of a multimodal approach for treatment-resistant cases.
Mechanisms of Action: Neurochemistry and Neuroplasticity
A frequent metaphor emerging from professional discussions is that medication provides the “hardware” fix, while psychotherapy rewrites the “software”. This analogy, while useful, simplifies the complex neurobiological interplay at work.
1. The Role of Medication: Symptom Stabilization Pharmacological agents, particularly SSRIs and antipsychotics, function primarily by altering neurotransmission to reduce acute symptom severity. This “symptom reduction” is not merely palliative; it is often a prerequisite for therapy. As noted in clinical discussions, a patient in the throes of acute mania or profound vegetative depression lacks the cognitive resources required for the introspection and learning inherent in Cognitive Behavioral Therapy (CBT) or psychodynamic work. Medication acts as a “floor,” stabilizing the patient enough to engage in the therapeutic alliance.
2. The Role of Psychotherapy: Structural Rewiring Contrary to the belief that therapy is solely “talk,” rigorous neuroimaging studies confirm that psychotherapy induces structural brain changes—a process known as neuroplasticity.
- Hippocampal Volume: Depression is associated with hippocampal atrophy. While antidepressants can arrest this loss, psychotherapy has been shown to restore functional neuroplasticity, effectively “rewiring” maladaptive neural circuits associated with fear and emotional regulation.
- Inter-Brain Plasticity: New models suggest that the therapeutic dyad itself triggers “inter-brain plasticity,” where the synchrony between therapist and client leads to lasting regulatory changes in the patient’s brain.
The Relapse Paradox: Long-Term Outcomes
A critical distinction must be made between response (feeling better now) and remission (staying well later). This is where the “medication only” approach often fails.
- Enduring Effects of Therapy: Research indicates that patients treated with CBT exhibit significantly lower relapse rates post-treatment compared to those treated with medication alone who subsequently discontinue use. The acquisition of compensatory skills—metacognition, emotional regulation, and behavioral activation—confirms that therapy confers a protective “prophylactic” effect that medication does not.
- The Maintenance Trap: A valid concern raised by clinicians is the indefinite nature of pharmacotherapy. Without the skills transfer provided by psychotherapy, patients often face a “revolving door” scenario where symptoms return immediately upon cessation of the drug.
Critical Analysis: The Biopsychosocial Imperative
The “medication versus psychotherapy” debate is a false dichotomy that ignores the biopsychosocial nature of mental illness. We must reject the reductionist view that mental health is exclusively biological (requiring only pills) or exclusively environmental (requiring only talk).
In clinical practice, we observe that biological interventions address the physiology of the disorder (sleep, appetite, agitation), while psychological interventions address the phenomenology (meaning-making, trauma processing, relational patterns). As evidenced by the “STAR*D” report and other major trials, the most effective clinicians are those who can skillfully titrate these interventions based on the patient’s specific presentation.
Conclusion
To advocate for one modality to the exclusion of the other is to practice with one eye closed. The synthesis of professional wisdom and empirical data points to a clear conclusion: while medication is often an indispensable tool for crisis stabilization and symptom management, psychotherapy remains the gold standard for long-term behavioral change and relapse prevention. As future psychologists, your task is not to choose a side, but to master the art of integration.
References
- American Psychological Association. (2017). Clinical practice guideline for the treatment of depression across three age cohorts.
- Cuijpers, P., et al. (2014). Adding psychotherapy to antidepressant medication in depression and anxiety disorders: A meta-analysis. World Psychiatry.
- Hollon, S. D., et al. (2005). Prevention of relapse following cognitive therapy vs medications in moderate to severe depression. Archives of General Psychiatry.
- Kandel, E. R. (1998). A new intellectual framework for psychiatry. American Journal of Psychiatry.
- Pampallona, S., et al. (2004). Combined pharmacotherapy and psychological treatment for depression: A systematic review. Archives of General Psychiatry.